
OCD and anxiety share a lot of surface features, but they work through different mechanisms and respond to different treatments. Anxiety tends to involve persistent worry about real-world situations. OCD centres on unwanted intrusive thoughts followed by compulsions, and it’s the compulsion-relief cycle, not the worry itself, that keeps the problem going.
This is one of the most common questions I hear. And it's a reasonable one, OCD and anxiety share a lot of surface features. Both involve worry. Both involve distress. Both can leave you exhausted from trying to manage thoughts you didn't ask for.
But they're not the same thing. They work differently, and they respond to different treatments. Getting the distinction wrong isn't a minor issue. In the UK, people wait an average of 6 to 7 years before accessing the right treatment for OCD, and in some cases, that's because OCD was being treated as generalised anxiety, with limited success (OCD Action, 2024).
This post explains the difference clearly, without jargon, and without suggesting one is somehow 'worse' than the other.
Key Takeaways
- In 2013, the DSM-5 reclassified OCD as separate from anxiety disorders, clinically, they are now in different diagnostic categories
- The core difference: OCD involves specific intrusive thoughts + compulsions; anxiety involves persistent worry about real-life concerns
-
UK research shows 62% of adults with OCD have at least one co-occurring anxiety or mood disorder (British National Psychiatric Morbidity Survey, NHS-commissioned)
-
In the UK, OCD goes untreated for an average of over 7 years, and the average age at which people first present to services is 29 (British Journal of Psychiatry)
- CBT with ERP is the gold-standard treatment for OCD; standard CBT with or without medication is first-line for GAD
Are OCD and anxiety actually separate conditions?
Since 2013, yes, formally. The DSM-5 moved OCD out of the anxiety disorders category into its own group: Obsessive-Compulsive and Related Disorders. That shift was based on evidence that the neurobiology, genetics, and treatment responses differ meaningfully from conditions like Generalised Anxiety Disorder (GAD).
That said, they frequently co-occur. UK research from the British National Psychiatric Morbidity Survey (NHS-commissioned) found that 62% of adults with OCD had at least one co-occurring condition, with anxiety disorders being the most common. So you can have both. What matters clinically is identifying which patterns are present, because that determines what treatment will actually work.
If any of this sounds familiar and you're wondering whether CBT might help, I offer a free 15-minute consultation — no pressure, just a conversation.
How does OCD actually work?
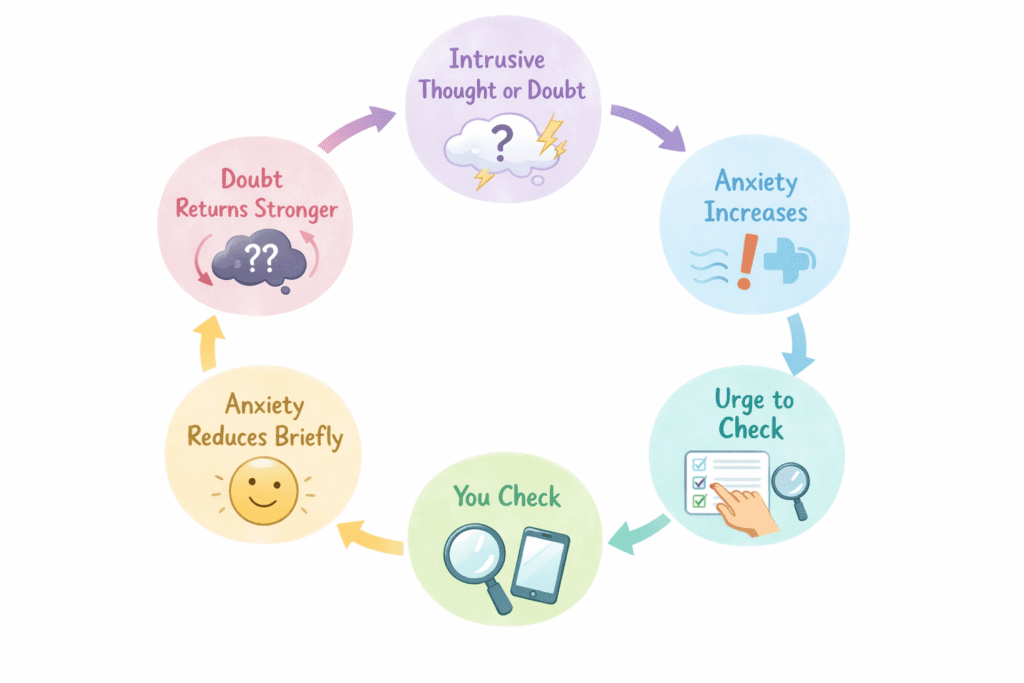
OCD runs on a specific, repeating cycle:
- Intrusive thought: an unwanted, distressing thought, image, or urge that feels alien or threatening
- Anxiety: the thought triggers significant distress
- Compulsion: an action (physical or mental) done to reduce the anxiety
- Temporary relief: the anxiety reduces briefly
- Return: the thought comes back, often louder than before
The intrusive thought is typically specific and ego-dystonic, meaning it feels completely contrary to who the person is. 'What if I hurt someone?' 'What if I said something offensive without realising it?' 'What if I'm secretly a bad person?' These thought horrifies the person having it.
Here's what makes OCD different from ordinary worry: the compulsion doesn't resolve it. Every time you perform a compulsion, you confirm to your brain that the thought was a genuine threat, and that a ritual was required to manage it. The OCD cycle deepens. The threshold for 'safe' rises.
If this cycle sounds familiar, CBT with a trained therapist can help you break it at the source — not just manage the anxiety, but change how your brain responds to the doubt in the first place.
How does generalised anxiety disorder work differently?
GAD looks and feels different in a few important ways. Where OCD fixates on specific intrusive thoughts paired with a compulsion, GAD tends to be a broader, more free-floating anxiety about real-life concerns; finances, health, relationships, work performance, the future in general.
Someone with GAD describes it as a background hum that never fully switches off. Worry pulls at them across multiple areas of life. It's not usually triggered by a specific thought they feel compelled to neutralize, it's more like a persistent low-level alarm that tracks real events, even if the response to those events is disproportionate.
GAD doesn't typically involve the obsession-compulsion cycle. There's no specific unwanted thought driving a specific ritual. There's worry that feels plausible, because it tends to attach to things that genuinely exist in the person's life.
The 5 key differences that matter clinically
Neither of these is a diagnosis, but these patterns can help clarify which direction you're looking in:
| Feature | OCD | Generalised Anxiety (GAD) |
| What triggers it | Specific intrusive thought, image, or urge | General real-life worries (finances, health, relationships) |
| Compulsions | Yes, always (physical or mental rituals) | No specific ritual; avoidance is common but not the same |
| How the thought feels | Ego-dystonic: feels alien, contrary to who you are | Ego-syntonic: feels like reasonable, if excessive, worry |
| Effect of checking/reassurance | Brief relief, then the thought returns stronger | Worry is persistent and pervasive, no ritual resolves it |
| Best treatment | CBT with ERP (Exposure and Response Prevention) | CBT, medication, or a combination, ERP is not the primary tool |
Why does this distinction matter for treatment?
Because the wrong treatment doesn't just fail, it can make OCD worse.
Standard CBT for anxiety teaches cognitive restructuring: examining thoughts, testing their accuracy, replacing unhelpful beliefs. For GAD, this works well. For OCD, it can function as a compulsion. The person tries to argue with the intrusive thought, analyse it, or reassure themselves that it isn't true. That's the OCD cycle in disguise, and it reinforces the problem.
ERP works differently. Instead of arguing with the thought, the person learns to sit with the anxiety without performing a compulsion, until it diminishes naturally. That process is what breaks the cycle.
Two-thirds of OCD patients who receive ERP show significant improvement; one-third achieve full recovery (OCD-UK, 2024). NICE guidelines (CG31) specifically designate CBT with ERP as the recommended treatment for OCD, separate from standard anxiety interventions, and the OCD Action Manifesto (2024) identifies treatment misalignment as a key driver of the estimated £5.1 billion annual cost of delayed and misdirected OCD care in the UK.
Treatment delays in the UK cost an estimated £5.1 billion annually (OCD Action, 2024). Getting the right diagnosis matters practically, not just clinically.

Signs it might be OCD rather than general anxiety
None of this replaces a proper assessment. But these patterns tend to lean toward OCD rather than generalised anxiety:
- You have specific, recurring thoughts that disturb or horrify you, particularly ones that feel completely unlike you
- You perform mental or physical rituals to neutralise the thought, even if you know logically it doesn't make sense
- The anxiety tracks a specific theme (harm, contamination, relationships, morality, religion) rather than general life concerns
- Reassurance or checking helps briefly, then the doubt returns, sometimes within minutes
If any of this sounds familiar and you're wondering whether CBT might help, I offer a free 15-minute consultation — no pressure, just a conversation.
Frequently asked questions
Can you have OCD and generalised anxiety at the same time?
Yes, and it's very common. Research from the British National Psychiatric Morbidity Survey (NHS-commissioned) found that 62% of adults with OCD had at least one co-occurring anxiety or mood disorder. Having both doesn't make treatment impossible; it means a good assessment will identify which condition to prioritise, and in what order.
My GP said I have anxiety. Could it actually be OCD?
Possibly. OCD is frequently misdiagnosed as generalised anxiety, particularly when the compulsions are mental rather than visible. If your anxiety seems to track specific, recurring themes, or if reassurance helps briefly and then the doubt comes back, it's worth asking for a specialist assessment rather than a general anxiety referral.
Is OCD more serious than anxiety?
Both conditions can be seriously debilitating. OCD is classified separately partly because it's harder to treat with standard anxiety approaches, not because it's inherently worse. The distinction matters for treatment, not for ranking suffering.
What should I do if I think I have OCD?
The most useful first step is speaking with a therapist who specialises in OCD. They can assess whether what you're experiencing fits an OCD presentation and recommend the most appropriate treatment. CBT with ERP has the strongest evidence base for OCD specifically, and it's available privately if NHS wait times are a barrier.
In summary
The honest answer to 'do I have OCD or anxiety?' is often 'possibly both.' What matters is identifying which patterns are at play, because that determines what treatment will actually help.
OCD isn't just anxiety with more rituals. It's a different condition with its own cycle, its own mechanisms, and a specific treatment approach that works. If you've been managing something that hasn't responded to standard anxiety support, it might be worth looking more carefully at whether OCD is in the picture.

Evelynne R. Scott-McFarlane
YOU MIGHT ALSO FIND HELPFUL
If you're finding it hard to tell whether what you're experiencing is OCD or anxiety, I offer a free 15-minute consultation, no commitment, just a conversation.