CBT and ERP for OCD: What Treatment Actually Involves
QUICK ANSWER
CBT (Cognitive Behavioural Therapy) for OCD is a structured, evidence-based psychological treatment that targets the thoughts, behaviours, and emotional responses that maintain OCD. Its core technique is ERP (Exposure and Response Prevention), in which clients gradually face feared situations while choosing not to carry out compulsive rituals, allowing the brain to learn that anxiety reduces without the compulsion. Both are recommended by NICE guideline CG31 as the first-line psychological treatment for OCD in the UK, and are recognised by the World Health Organisation. CBT for OCD is the full treatment programme: assessment, psychoeducation, formulation, ERP practice, and relapse prevention. ERP is the active ingredient within that programme that directly breaks the OCD cycle. They are not interchangeable terms, but in practice they are delivered together by a specialist therapist, usually a BABCP-accredited practitioner in the UK.
KEY TAKEAWAYS
- CBT for OCD and ERP are not the same thing, but they belong together. ERP is the core active technique within CBT for OCD. You cannot do good CBT for OCD without ERP, and ERP without the CBT framework produces weaker long-term outcomes.
- CBT for OCD is fundamentally different from CBT for depression or generalised anxiety. Techniques used for other conditions, particularly thought-challenging, can actively make OCD worse if applied incorrectly.
- NICE guideline CG31 recommends CBT including ERP as the first-line psychological treatment for OCD in adults, children and young people. This recommendation has been in place since 2005 and was reconfirmed in the 2019 surveillance review.
- A systematic review and meta-analysis of randomised controlled trials found that CBT with ERP produced large effect sizes, with around 67% of participants achieving recovery status at the end of treatment (PubMed, 2021). Treatment gains were durable at follow-up.
- OCD affects approximately 750,000 people in the UK at any one time (OCD-UK). The right treatment makes a significant difference. The wrong treatment, or generic CBT not tailored to OCD, does not.
- Recovery from OCD is not about eliminating intrusive thoughts. It is about ending the compulsions that give those thoughts their power.

Most people who find their way to this article already know something is wrong. They have read about OCD, perhaps recognised themselves in it, and started looking for what actually helps. They may have come across the terms CBT and ERP and wondered what the difference is, which one they need, and what any of it looks like in practice.
These are exactly the right questions to be asking. CBT and ERP are the two treatments that the evidence points to consistently. They are also two terms that are frequently confused with each other, sometimes used interchangeably, and not always well explained even by those recommending them. If you have ever left a GP appointment with a referral for "CBT" and wondered whether that actually meant ERP, or whether you were getting the right thing, that confusion is understandable.
This article covers both: what CBT for OCD is, what ERP is, how they fit together and how they differ, what a course of treatment actually looks like week by week, and what recovery genuinely means. By the end, you will have a clear picture of what good OCD treatment involves and what to look for when you seek it.
What Is CBT for OCD?
CBT (Cognitive Behavioural Therapy) for OCD is a structured, evidence-based psychological treatment that targets the specific cycle maintaining OCD: the intrusive thought, the anxiety it creates, the compulsion performed to reduce that anxiety, the brief relief, and the sensitisation that brings the whole thing back, worse than before. That cycle is what CBT for OCD is designed to interrupt.
It is not simply "CBT." This distinction matters more than it might appear. CBT is a broad family of therapies used across many different conditions, and the techniques used for depression or generalised anxiety are not the same as the techniques used for OCD. In fact, one of the most common reasons people with OCD fail to improve in therapy is that they receive generic CBT rather than OCD-specific CBT. The techniques intended to help can, when applied without this distinction, actively feed the OCD cycle instead of breaking it.
The clearest example is thought-challenging. In CBT for depression or anxiety, examining the evidence for and against an unhelpful thought is genuinely therapeutic. In OCD, doing the same thing, asking whether a feared outcome is likely, reasoning through whether the intrusive thought makes sense, engaging with the content of the thought in any way, is itself a compulsion. It provides brief relief and reinforces the very cycle it is trying to undo.
CBT for OCD therefore works differently. The goal is not to challenge your intrusive thoughts or to replace them with more accurate ones. The goal is to change your relationship with the thoughts: to encounter them without treating them as commands that require a response. That shift, from a thought being something you must act on to something you can notice and let pass, is what the treatment builds towards.
A full course of CBT for OCD includes the following phases, all of which work together. It is the complete architecture that produces lasting change.
- Assessment: A thorough exploration of your OCD history, current triggers and compulsions, how much of daily life is affected, and what has and has not helped previously. This is collaborative, not clinical in the distant sense. It is the beginning of building a shared understanding of what is happening for you specifically.
- Psychoeducation: Your therapist explains the OCD cycle clearly: how intrusive thoughts arise, why compulsions maintain anxiety rather than resolving it, what ERP involves and why it works. Understanding the mechanism matters. You are not being asked to do something counterintuitive blindly. You are being asked to do it with a clear rationale in place.
- Formulation: Together, you build a personalised map of your OCD, specific to how it operates for you. Your triggers, the thoughts that follow, the compulsions or mental rituals you use to manage the distress, the relief they bring, and the way the cycle resets. This formulation is the foundation everything else builds on.
- ERP: The active treatment phase. This is where the real work happens, and it is covered in full in the next section.
- Between-session tasks: Progress in CBT for OCD depends on what happens between sessions. Your therapist sets agreed tasks that extend the work into daily life. These are reviewed without judgement and used to refine the approach week by week.
- Relapse prevention: In the final phase of treatment, sessions focus on consolidating what has been learned: what to do if OCD resurfaces during a stressful period, how to recognise early warning signs, and how to apply what you have learned independently, without needing to return to therapy every time.
The NHS recommends CBT as the primary psychological treatment for OCD. Mind UKspecifically notes that the CBT recommended for OCD should include ERP. The two are inseparable in good clinical practice.
The number of sessions required depends on the severity of your OCD. NICE guidelines recommend up to 10 therapist hours for mild functional impairment, and more intensive treatment for moderate to severe presentations. For severe OCD, combined treatment with an SSRI and CBT including ERP is recommended.
What Is ERP Therapy?
Exposure and Response Prevention (ERP) is the core active technique within CBT for OCD. It is a structured process in which a person gradually encounters the situations, thoughts, or feelings that trigger their OCD (the exposure) while deliberately choosing not to carry out the compulsive ritual or mental behaviour that would normally follow (the response prevention).
The definition used by NICE and endorsed across the clinical literature is as follows: ERP works by having clients gradually face feared situations while refraining from compulsive behaviours, so the brain learns that anxiety reduces naturally without the compulsion being performed.
This is a significant shift from what most people expect treatment to involve. Most people arrive hoping that therapy will make the intrusive thoughts go away, or teach them to manage anxiety so that it never gets too high. ERP does neither of these things, and this is precisely why it works. Instead of providing relief from the anxiety, it allows the anxiety to rise, peak, and then fall of its own accord. Every time that happens without the compulsion, the brain receives new information: the feared outcome did not materialise, the anxiety was survivable, and the ritual was not what kept you safe.
The theoretical basis for ERP rests on two processes. The first is anxiety habituation, the well-established finding that anxiety naturally decreases when a feared situation is encountered without escape, given enough time and enough repetitions. The second, and more recent, is inhibitory learning: ERP does not erase the original fear association but builds a new, competing association alongside it. The intrusive thought can arise without automatically triggering the compulsion. The gap between thought and behaviour widens. That gap is what recovery feels like from the inside.
ERP is not a new or untested approach. A systematic review and meta-analysis of randomised controlled trials published in peer-reviewed research (2021) found that CBT with ERP produced large pooled effect sizes across all comparison conditions, with around 67% of participants meeting recovery criteria at the end of treatment, and gains maintained at follow-up. The OCD-UK charity describes ERP as the most effective psychological treatment available for OCD.

How CBT and ERP Fit Together: Understanding the Difference
Because ERP is always delivered within a CBT framework, the two terms are often used as though they mean the same thing. They do not, and it is worth being precise about this, both for your own understanding and because it affects what you should be looking for in a therapist.
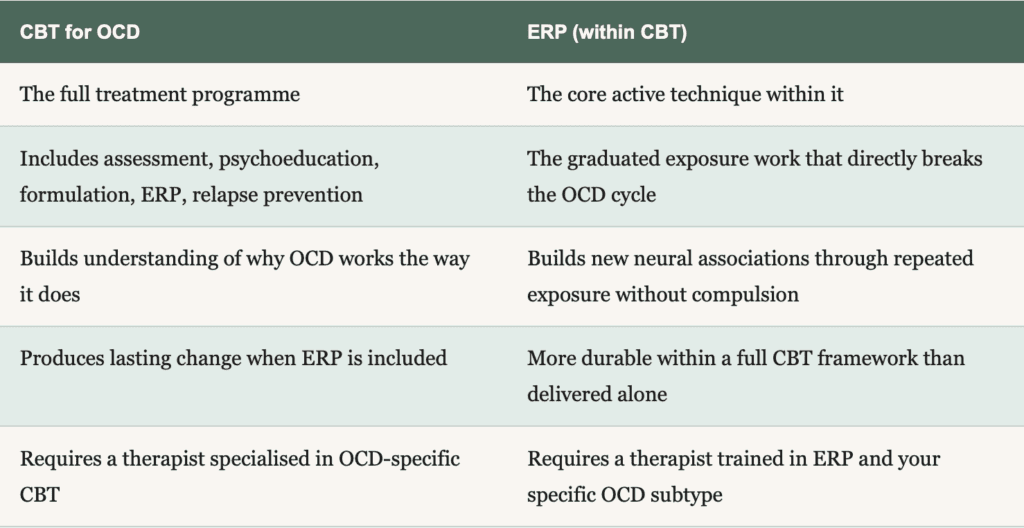
The simplest way to understand the relationship is this: CBT for OCD is the full treatment programme. ERP is the central technique within that programme that does the direct work of breaking the OCD cycle. CBT provides the context, the rationale, the formulation, the cognitive framework for understanding your OCD, and the relapse prevention scaffolding. ERP provides the lived experience of sitting with anxiety without compulsions, which is what changes the cycle at a neurological level.
Why does this distinction matter practically? Because if a therapist offers you "CBT for OCD" but focuses primarily on discussing the content of your thoughts, or offers reassurance as part of the sessions, or never builds a fear hierarchy or guides you through exposure exercises, you are not receiving the evidence-based treatment for OCD. You are receiving something else. It may be helpful in other ways. It will not break the OCD cycle.
Equally, ERP without the broader CBT framework can leave people with insufficient understanding of why they are doing what they are doing, less ability to generalise the learning to new situations, and less preparation for managing OCD independently when treatment ends. The research supports the combined approach.

CONSIDERING TREATMENT?
Ready to find out if this is right for you?
CBT and ERP work — but the process looks different for everyone. A free consultation is a good place to start. No pressure, just a chance to talk through your situation.
No referral needed · Sessions £100
BABCP Accredited · Online · London & UK
What Sessions Actually Look Like
Most people's anxiety about starting therapy comes from not knowing what it involves in practice. The name suggests something will be forced on you. It will not be. Therapy is always collaborative, always graduated, and always guided. Here is what the process looks like from the inside.
Building your fear hierarchy
Before any exposure begins, you and your therapist construct a personalised fear hierarchy together: a ranked list of your OCD triggers, from those that produce mild to moderate anxiety all the way to those that feel currently unmanageable. Each item is given a rough distress rating out of 10. Nothing goes on this list without your agreement. It is a working document, not a fixed prescription, and it gets adjusted as treatment progresses.
For someone with contamination OCD, the hierarchy might begin with touching a door handle at home and move gradually towards using a public toilet without washing. For someone with harm OCD, it might begin with holding a knife while preparing food, or leaving the house without checking the gas. For someone with Pure O, the hierarchy targets mental compulsions: the reviewing, the replaying, the reassurance-seeking from others, the mental neutralising. The principle is the same regardless of OCD subtype. ERP works across all forms of OCD, including those where the compulsions are primarily internal.
Starting in the middle, not at the top
ERP does not begin with the most feared item on your hierarchy. It begins somewhere in the mid-range: something that produces meaningful anxiety but feels survivable. Items that produce no anxiety at all teach the brain nothing new. Items that produce overwhelming anxiety make it harder to stay present in the exposure long enough for learning to occur. The starting point is chosen carefully, and it is chosen together.
Sitting with the anxiety without the compulsion
This is the part that feels most counterintuitive, and it is the part that matters most. When anxiety rises during an exposure, the trained response is to perform the ritual. ERP involves choosing not to do that. You stay with the discomfort, let the anxiety curve do what it does naturally: rise, peak, and fall. Your therapist is present throughout in-session exposures. They are not observing from a distance. They are coaching you through it, helping you stay engaged rather than escape mentally.
Every time you remain with the anxiety without the compulsion, the brain receives new information. The feared outcome did not happen. The anxiety reduced without the ritual. The compulsion was not what kept you safe. That information accumulates. The hold of the OCD loosens.
Addressing "Won't this make my anxiety worse?"
Almost everyone asks this before they begin ERP. The honest answer is that within individual exposures, anxiety will temporarily increase. That is by design. The anxiety needs to rise for the brain to have the opportunity to learn it can fall again without the compulsion. This is not gratuitous discomfort. It is the mechanism through which the cycle changes.
The trajectory of a full course of ERP, however, is a progressive reduction in OCD severity over weeks. The NHS acknowledges that ERP can feel challenging at the start, and the pace can always be adjusted. A well-trained ERP therapist will never push you beyond what you can work with at a given moment. Challenge is part of the process. Overwhelm is not.

What Does Recovery from OCD Look Like?
Recovery from OCD is not the absence of intrusive thoughts. It is worth saying that plainly, because for many people that is the benchmark they are holding, and it makes recovery feel permanently out of reach. Intrusive thoughts are a normal part of human cognition. Research consistently shows that the vast majority of people experience unwanted, distressing intrusive thoughts. The difference between someone with OCD and someone without it is not the presence of the thoughts but what happens next: the meaning assigned to them, and the compulsions that follow.
CBT and ERP do not eliminate intrusive thoughts. What they change is your relationship with them. A thought arises and instead of triggering an automatic anxiety spike and a compulsion, it passes through like background noise. It loses the charge that made it feel like an emergency demanding a response. That shift does not happen through insight or willpower. It happens through practice: hundreds of small moments of choosing not to perform the compulsion, until the new response becomes the default.
In practical terms, recovery looks like:
- spending significantly less time on compulsions or mental rituals each day
- being able to tolerate uncertainty without needing to resolve it immediately
- making choices based on what you want to do, not what OCD is demanding
- noticing intrusive thoughts without being pulled into them
- getting back hours, attention, and energy that OCD was previously consuming
The Royal College of Psychiatrists notes that most people who complete a course of CBT including ERP experience a significant reduction in symptoms. Research shows around 67% meet recovery criteria at the end of treatment, with improvements sustained at follow-up. OCD can resurface during periods of stress or major life change, which is why relapse prevention is built into every course of good CBT for OCD. If symptoms return, you have the tools to respond quickly rather than feeling back at the beginning.
Related Articles: How to Stop Intrusive Thoughts, Without Fighting Them
What Can Actually Help?
Both health anxiety and OCD are genuinely treatable conditions. The evidence supporting CBT as an effective psychological approach for both is consistent and well-established (NICE CG31). Recovery is possible, and for most people it does not require years of therapy.
The most important first step is understanding what you are actually dealing with. That clarity changes everything, because it means the work in therapy is aimed in the right direction from the start.
Frequently Asked Questions
READY TO TAKE THE NEXT STEP?
Ready to start CBT for OCD?
Now you know what treatment involves, the next step is finding out if it's right for you. Book a free consultation to talk through your symptoms and what working together would look like.
ABOUT THE AUTHOR
Who writes this?

Evelynne R. Scott-McFarlane
BABCP ACCREDITED CBT THERAPIST
I'm a BABCP accredited CBT therapist specialising in anxiety - OCD, health anxiety, and panic disorder. I trained at King's College London and work online with clients across London and the UK.
I write these articles because good information is hard to find. Most mental health content online is either too vague to be useful or too clinical to be readable. I'm trying to do something different
![]()
![]()



